The Big Idea — one disturbed capacity
Chapters 4–6 explained aphasia by localising functions in many separate centres; Chapter 7 replaced that with a hierarchy of levels. Chapter 8 takes a third path: trace the whole variety of aphasic symptoms back to a disturbance of a single functional capacity.
A global (or single-factor) model explains the apparent variety of aphasic signs as the effect of a disturbance of one underlying capacity. For Pierre Marie that factor is a disorder of general intelligence; for Kurt Goldstein it is the loss of the "abstract attitude." The two are methodologically opposite — Marie's case is anatomical, Goldstein's is psychological.
Where this chapter sits — the four approaches
| Chapters | Approach | Core idea |
|---|---|---|
| 4–6 | Connectionist | centres for functions, joined by connections (localizationist). |
| 7 | Hierarchical | successive levels of the nervous system; higher modulate lower. |
| 8 (this) | Global / holist | one disturbed functional capacity underlies all aphasic signs. |
| 9 | Process | no single component carries out a whole psychological function. |
Global models are a kind of holist theory: like the hierarchical models, they reject the connectionists' discrete cortical centres and seek one unifying principle behind the many symptoms. These are the last of the "clinical" models the book considers before turning to process and linguistic approaches.
Both men accepted that several aphasic syndromes exist; neither literally claimed that one factor could describe every manifestation of aphasia. Their distinctive contribution is the emphasis each placed on a single underlying factor.
But note the asymmetry: Marie effectively pushed it all the way — "there is only one aphasia" — so for him the single factor very nearly is everything. Goldstein, by contrast, explicitly never claimed a single disorder accounted for all of aphasia. Stating this distinction is what separates a top answer from a vague one.
The two global models, side by side
| — | Pierre Marie (1906) | Kurt Goldstein (1948) |
|---|---|---|
| Single factor | a disorder of general INTELLIGENCE (with comprehension) | loss of the ABSTRACT ATTITUDE |
| Account is… | anatomical / vascular | psychological (gestalt / organismic) |
| Output explained by | a separate subcortical motor disorder — "anarthria" | failure to assume the abstract attitude in the task |
| Neural basis | dominant temporo-parietal area (+ quadrilateral space) | integrated activity of much of the brain (both hemispheres) |
| Single factor = ALL aphasia? | effectively YES ("only one aphasia") | NO — never claimed it explained everything |
| Signature | "Broca's = Wernicke's + anarthria" | concrete vs abstract attitude; "catastrophe" avoidance |
In the 2023–2025 papers, "global models" never appeared as a stand-alone direct question — it was examined in 2024 (Q3) as a comparison: "Differentiate between Hierarchical models and Global models." But the examiner asks "Discuss the X models of aphasia" for the other traditions, so a direct "Discuss the global models" is a very plausible parallel. Prepare both forms — the Cheatsheet has the comparison ready-made.
→ Work through Pierre Marie, the Marie–Dejerine controversy, and Kurt Goldstein, then consolidate in the Cheatsheet and prove it in the Self-Test.
Pierre Marie (1906) — "There is only one aphasia"
In a set of widely publicised, highly controversial papers, Marie argued that the entire connectionist project of sorting aphasics into clinical sub-types was an error. His account is anatomical and intellectual — and it is built from three moves: a thesis about intelligence, a theory of output ("anarthria"), and a vascular argument.
There is only one true aphasia, and it is Wernicke's aphasia: comprehension of language is disturbed as part of a more general deficit in general intelligence. The responsible lesion lies in the posterior brain — particularly the temporo-parietal junction of the dominant hemisphere.
Marie knew that not every aphasic shows an obvious comprehension problem, so he argued the deficit could be mild and detectable only by demanding tests. His later refinement (Marie 1908) defined the capacity more precisely as one involving both language and "ideas learned in a didactic fashion" ("certaines idées apprises de façon didactique").
"Of the three pieces of paper that I have put before you, take the largest and crumple it into a ball, put the smallest in your pocket, and take the middle one and fasten it to the window."
In over 100 consecutive aphasics (many with the anterior syndrome), not one could carry out such a three-step command properly — which, Marie held, shows that the general intelligence it requires is impaired in all true aphasia.
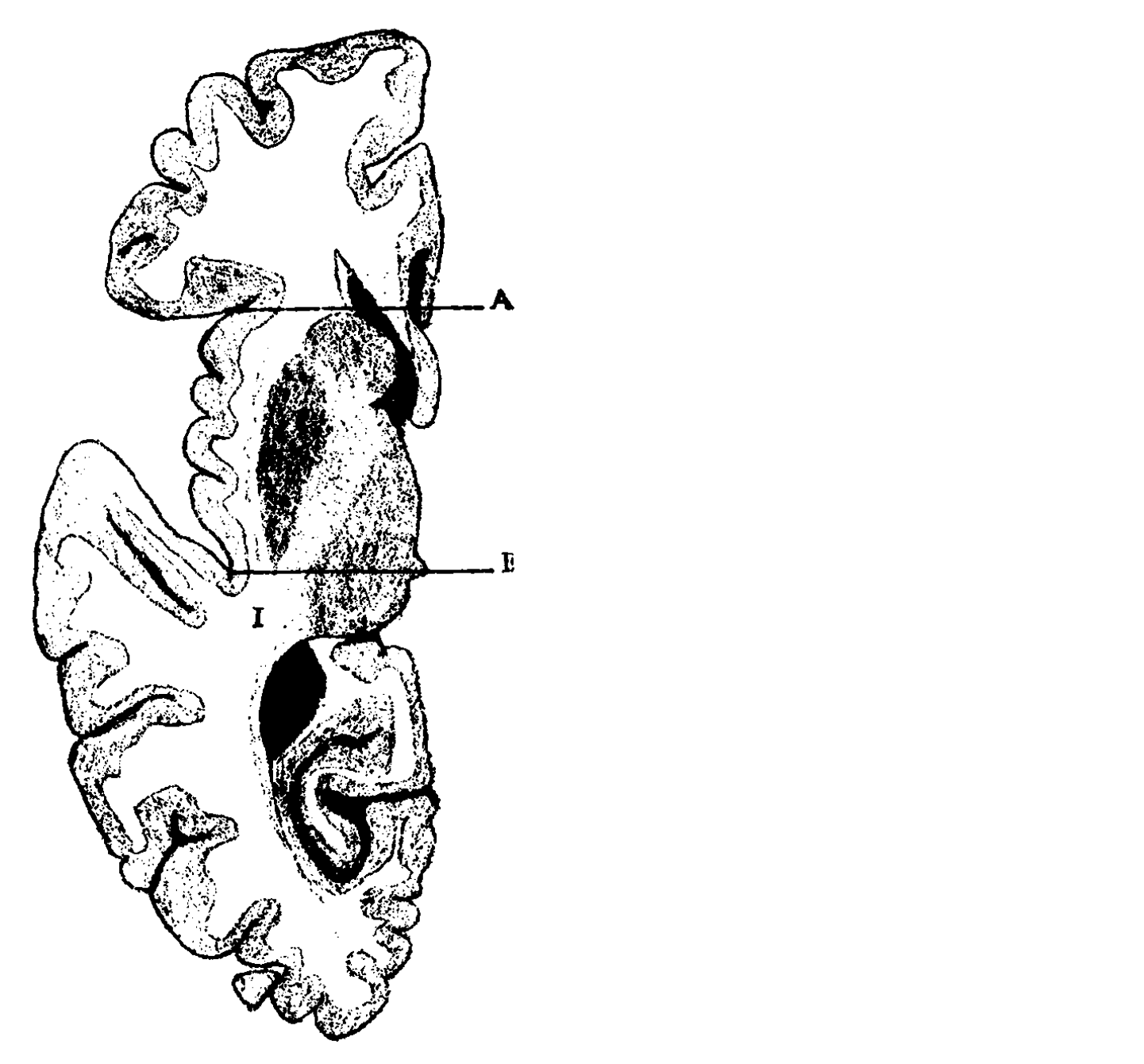
2 · Anarthria & the "quadrilateral space" — explaining the output (Fig 8-1)
What, then, of the obvious difference in speech output between anterior and posterior patients? Marie denied this was due to a cortical speech-planning centre. It was, he said, a disturbance of the motor apparatus itself, and the lesion responsible was subcortical. (Anterior aphasics, he noted, always have some impairment of the facial/swallowing muscles; minor impairment shows up only in the most complex movements — i.e. speech.) Click each card to study the figure:
Click a card above to read the detail.
"There is only one aphasia: Broca's aphasia is Wernicke's aphasia plus anarthria."
In other words, what others called Broca's aphasia is simply the one true (Wernicke-type) aphasia complicated by a separate, subcortical motor disorder of articulation.
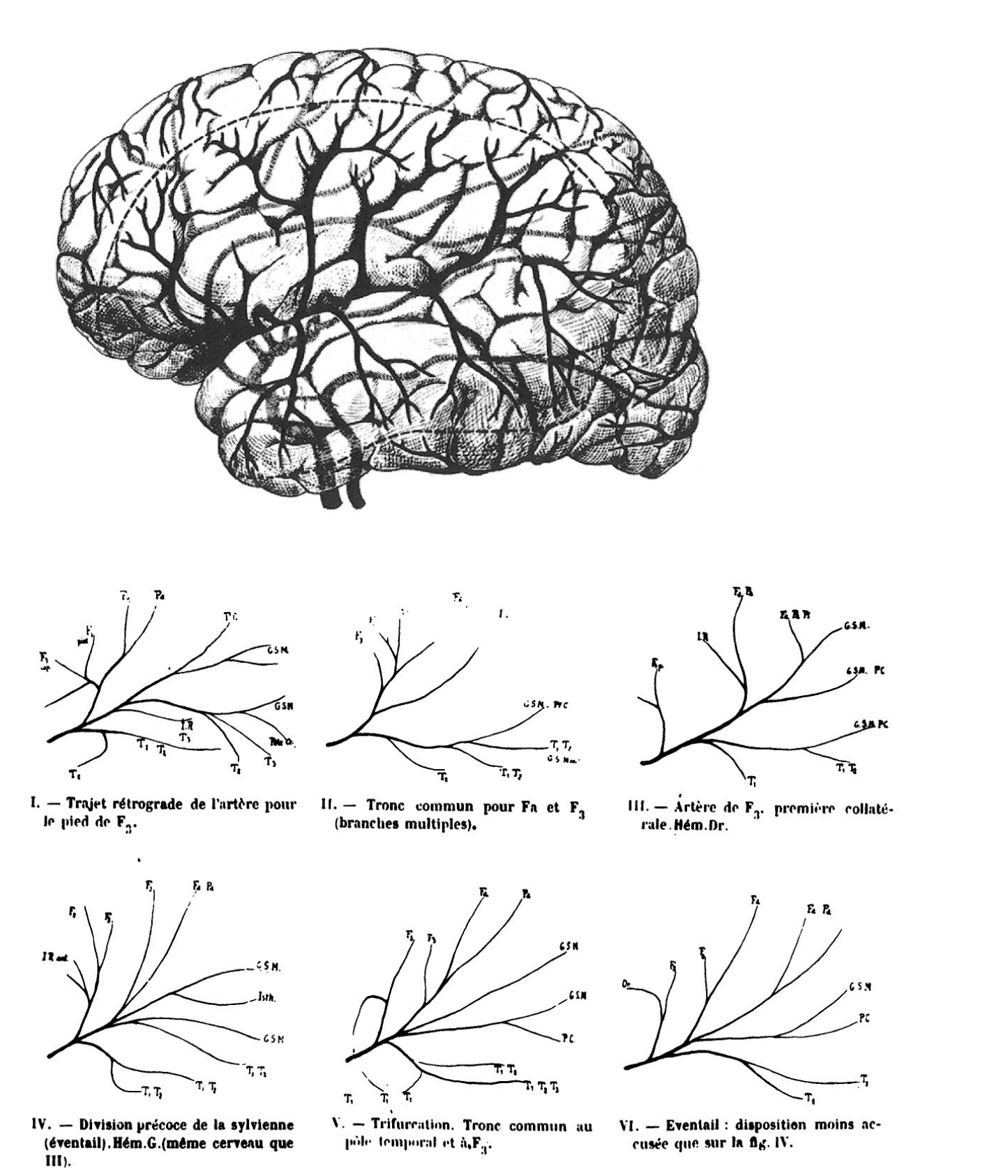
3 · The vascular argument — Marie's lasting contribution (Fig 8-2)
Marie's most durable contribution was neither the slogan nor the intelligence theory, but his account of the blood supply of the language zones — how vascular lesions produce the clinical varieties of aphasia. Click each card:
Click a card above to read the detail.
4 · Re-examining Broca's own patients — the dramatic evidence
In a dramatic flourish, Marie re-examined the brains of Broca's own original patients:
The lesion extended back as far as the supramarginal gyrus (parietal) and deep into the white matter — which, Marie argued, confirmed that Broca's aphasia involves a posterior lesion and discredited the anterior-only account.
Marie claimed there was no focal lesion at all — only the diffuse atrophy seen in senile degeneration.
This is less convincing than it seemed in 1906. Broca did appreciate the posterior extent of Leborgne's lesion, and based his theory on correlating the severity of different parts of the lesion with the stages of the patient's deficits — so the re-examination didn't really overturn Broca's reasoning.
5 · Moutier's thesis (1908) — the evidence base
The most extensive evidence for Marie's view came not from Marie but from his student François Moutier, whose medical thesis is one of the most extensive reviews of an aphasic syndrome ever published.
- Bibliography alone = 67 printed pages; 387 cases from the literature + 44 of his own (24 studied clinically and with autopsies).
- Used serial microscopic sectioning (technique perfected by the Dejerines, 1901) — up to ~2,000 slices through a single hemisphere.
- Findings marshalled for Marie: 7 Broca's aphasia without a third-frontal lesion; 12 lesions in Broca's area without Broca's aphasia; 5 Broca's aphasia with a lenticular / quadrilateral lesion.
Threatened by his student's abilities, Marie later blocked Moutier's career. Moutier abandoned the brain for "the folds of the intestine," became France's leading academic gastroenterologist, and pioneered the gastroscope (story told by Lecours & Joanette 1984).
6 · Marie's rhetoric
Marie's panache guaranteed attention. He titled his first major paper "The left third frontal convolution plays no special role in the faculty of language" — a broadside at the most deeply held "truth" of French neuropsychology — and implied that Broca's theory had been accepted as much for the academic-political milieu (Bouillaud's influence in French neurology) as for any intrinsic scientific merit.
The Marie–Dejerine Controversy (1908)
Marie's broadside could not go unanswered. A sharp controversy with Jules Dejerine (whose work on alexia-without-agraphia appears in Ch. 5) climaxed in three "discussions" sponsored by the French neurology society in the summer of 1908 (Klippel 1908) — covering clinical description, pathological anatomy and pathophysiology. The two protagonists, with their students and collaborators, disagreed on almost every important point.
Meeting 1 — clinical matters (especially Broca's aphasia)
Both restated their views on comprehension. Dejerine held that Broca's aphasics have only a mild verbal deafness, and that their "verbal blindness" appears only for longer structures — an association problem, not a true alexia. Marie insisted that Broca's and Wernicke's aphasics differ only in degree, not in kind in their receptive impairment.
The sharpest clash was over output. Dejerine drew a careful distinction; Marie rejected it:
| Dejerine's distinction | Profile & cause |
|---|---|
| Dysarthria | mispronounces ALL words but retains the usual word inventory; from paralytic / spastic / ataxic disturbances of the speech organs. |
| Motor aphasia | pronounces words well but uses a reduced stock of words; a psychological impairment of the representation of words. |
The distinction is not clear-cut — many patients show both a reduced word-stock and mispronunciation. Only disturbances of "internal language" are truly aphasic, he said, and these are similar in all forms of aphasia. (The disciple André Thomas added clarifications; neither protagonist convinced the other.)
Meeting 2 — anatomy: the decisive blow
The second discussion dealt with the anatomical basis of language, and proved decisive. Its most memorable moment was the demonstration by Augusta Klumpke Dejerine — Jules Dejerine's wife and collaborator.
Presenting microscopic sections of the normal brain, she showed that:
- Broca's area (the pars opercularis + triangularis of the third frontal convolution) does NOT lie anterior to Marie's quadrilateral space, as Marie had maintained — it lies just lateral to it; and
- the white-matter fibres to and from Broca's area pass through the antero-superolateral portion of the quadrilateral.
The implication is fatal for Marie. A subcortical lesion causing anarthria therefore affects exactly these Broca's-area fibres — just as a lesion of the internal capsule causes hemiplegia by interrupting the descending motor tract (relating it to the motor-strip cells). This accounts for subcortical dysarthria without denying the importance of Broca's area in speech. Marie tried to redefine his zone, but could not point to any fibre-free subcortical region in which a lesion caused anarthria — and his position was badly undermined.
Broca's second case was produced and examined. Dejerine saw a lesion in the third frontal convolution; Moutier (Marie's representative) saw "only a few scratches." Neither side would have the brain cut then and there → the question remained unsettled.
The verdict on Marie
- He never adequately characterised the "general intelligence" he invoked.
- Subsequent work shows aphasic comprehension disorders differ qualitatively, not just quantitatively (Chs 12–16).
- Many aphasic abnormalities are now understood as disorders of a purely linguistic system — not by-products of an intellectual or motor disorder.
But Marie's lasting impact (legacy)
Yet Marie's impact was real. Head (1926) called him an "iconoclast" who cast serious doubt on the connectionist taxonomies. After 1906:
- there was far greater emphasis on detailed description of aphasic syndromes;
- the existence of a comprehension deficit in Broca's aphasia — noticed before but conveniently ignored — could no longer be brushed aside.
To what extent are intellectual and sensory-motor disorders allied to — if not responsible for — aphasic symptoms? Investigated continuously since 1906; answers are still not clearly forthcoming.
Kurt Goldstein (1948) — gestalt & the "abstract attitude"
Marie's failure didn't settle whether some unitary explanation of aphasia was possible. Goldstein's major work, Language and Language Disturbances (1948), drew together contemporary linguistics, psychology and neuropsychology — and made the loss of the "abstract attitude" the central explanatory concept. Unlike Marie, he never claimed a single disorder explained all of aphasia.
1 · Influences & background
- Accepted Jakobson's analysis of phonemic breakdown and the hierarchical approach (Ch. 7).
- Discussed "inner speech" — a self-regulatory use of language studied by Vygotsky (1939); a disturbance of it = his "central" aphasia, which closely corresponds to the connectionists' conduction aphasia.
- But his deepest influence was gestalt psychology.
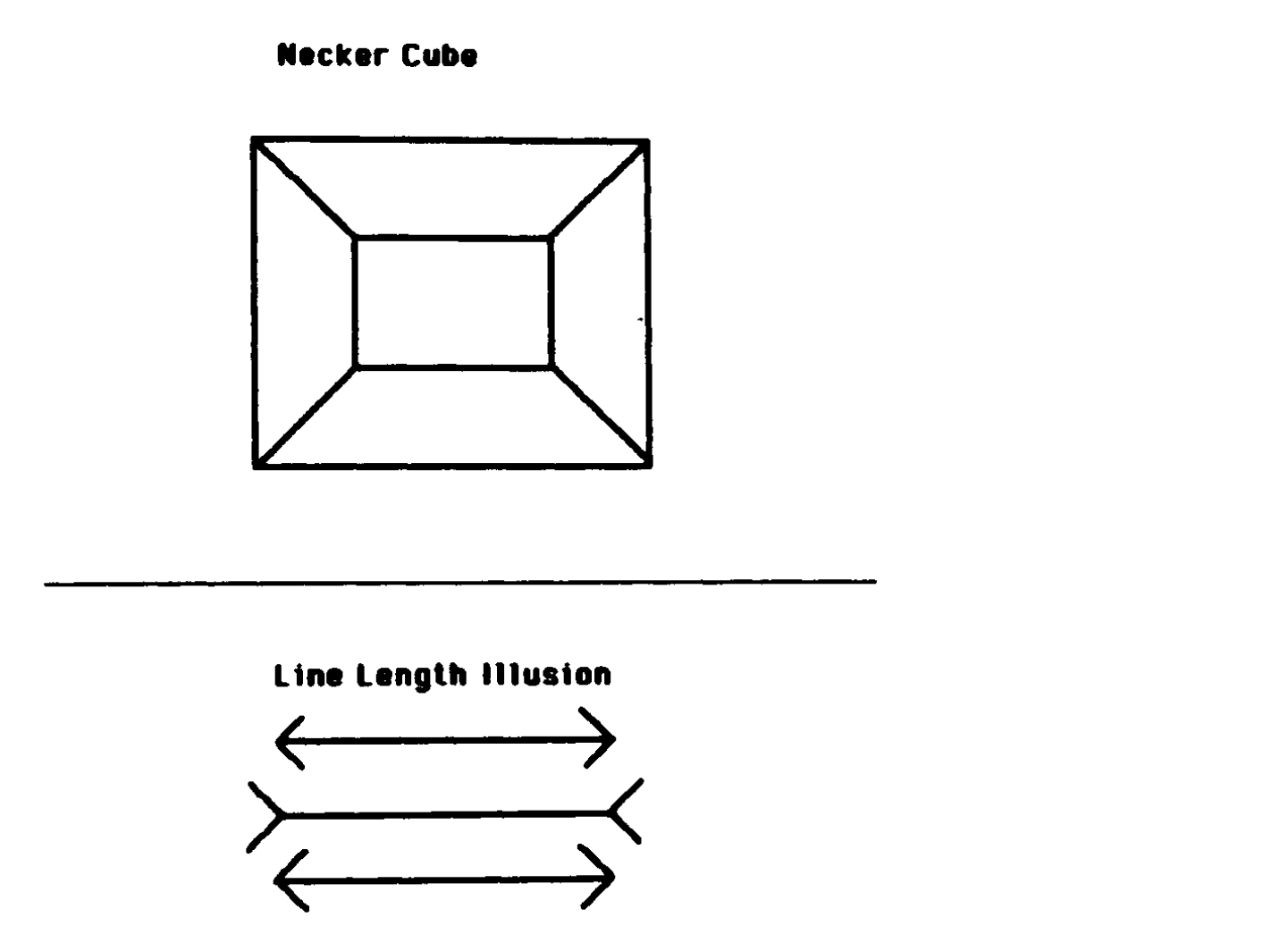
2 · Gestalt & the "organismic view" (Fig 8-3)
Gestalt psychology stressed two things: (1) the contribution the organism itself makes to perception, cognition, memory and action; and (2) the integrated nature of its psychological states. Its favourite demonstrations were perceptual. Click each card:
Click a card above to read the detail.
3 · Four mechanisms by which brain disease impairs function
Goldstein distinguished four ways a brain lesion produces functional impairment:
| # | Mechanism | Goldstein's term | Examples / notes |
|---|---|---|---|
| 1 | Damage to a brain area | "direct" (= Jackson's negative) | six lesion-effects — see the box below. |
| 2 | Separation of an undamaged area from a damaged one (disinhibition) | part of Jackson's positive effects | e.g. increased tendon reflexes; logorrhea. |
| 3 | A damaged area's remote effect on intact tissue = DIASCHISIS (von Monakow 1914) | "indirect" | e.g. improvement after removing a frontal-lobe scar → therapeutic value of removing/disconnecting inhibitory damaged tissue. |
| 4 | Avoidance of "catastrophe" by the integrated patient | "protective mechanisms" | orderliness, avoiding novelty, needing structure; explains day-to-day variability (e.g. lined vs unlined paper). |
Physiological (3): (i) a raised threshold for neuronal excitation; (ii) abnormal lability of that threshold; (iii) abnormal duration / spread of excitation.
Psychological (3): (iv) increased sensitivity to external stimuli; (v) difficulty maintaining sharp figure–ground boundaries; (vi) impaired adoption of the "abstract attitude" — the most important by far.
A "catastrophe" is a performance failure marked by disorder, disharmony and anxiety, which the patient seeks to avoid via "protective mechanisms." This explains the day-to-day variability Head had emphasised: a patient may write on lined paper (the lines give enough structure to initiate the act) but not on unlined paper (unable to decide where to begin, he may not try at all).
4 · The abstract attitude — the central concept
Concrete: we are passively bound to the immediate, specific situation — we enter a dark room and simply push the button for light.
Abstract (also categorical / conceptual): we transcend the immediate — we desist from the button, reflecting that we might wake someone asleep. We consider the situation conceptually; the particular thing becomes a mere example of a "category."
The abstract attitude underlies six potentialities (Goldstein 1948: 6):
- assuming a mental set voluntarily; taking initiative; beginning a performance on demand;
- shifting voluntarily from one aspect of a situation to another; making a choice;
- keeping various aspects in mind simultaneously; reacting to two stimuli not intrinsically together;
- grasping the essentials of a whole; breaking it into parts and recombining them;
- abstracting common properties; planning ahead ideationally; an attitude toward the "merely possible"; thinking / performing symbolically;
- detaching the ego from the outer world.
5 · Applying it to aphasia
Goldstein ascribed a great range of aphasic symptoms to the inability to assume the abstract attitude toward a linguistic structure or its use:
- Phonemic dissolution (after Jakobson): voiced vowels and consonants require more "voluntary attention" than voiceless segments → they require the abstract attitude → they are lost first.
- Naming disorders; the intellectual disorders that accompany aphasia.
- The selective loss of the "little" / grammatical words — a contrast that returns in modern work on agrammatism (Ch. 15).
6 · Critique
It is best known for its gestalt framework and for insisting that the abstract attitude be assessed in clinical diagnosis — but it is unclear how a single breakdown explains all the specific deficits. It seems almost contradictory that losing one capacity yields both anomia (a content-word problem) and agrammatism (a function-word problem).
Goldstein himself admitted breakdown can be domain-specific (each domain needing its own description), and — as Geschwind (1964) noted — he largely accepted the standard symptom–lesion correlations (localization), even while disputing the mechanism of symptom creation.
He identified his work as a continuation of Jackson, Marie and Head — using "de-differentiation" of neuropsychological function, integrated performance by a lesioned organism, and the ubiquity of the effects of losing a single capacity (the abstract attitude).
Cheatsheet
Everything condensed. Anchor the chapter on two hooks: Marie's slogan ("Broca's = Wernicke's + anarthria") and Goldstein's concrete vs abstract attitude.
Marie vs Goldstein — side by side
| Dimension | Pierre Marie (1906) | Kurt Goldstein (1948) |
|---|---|---|
| Single factor | disorder of general INTELLIGENCE (with comprehension) | loss of the ABSTRACT ATTITUDE |
| Method | anatomical / vascular | psychological (gestalt / organismic) |
| Output explained by | a separate subcortical motor disorder — anarthria | failure to adopt the abstract attitude in the task |
| Neural basis | dominant temporo-parietal area (+ quadrilateral space) | integrated activity of much of the brain (both hemispheres) |
| One factor = ALL aphasia? | effectively YES ("only one aphasia") | NO — never claimed it |
| Signature | "Broca's aphasia = Wernicke's aphasia + anarthria" | concrete vs abstract attitude; "catastrophe" avoidance |
The three-way contrast — Connectionist vs Hierarchical vs Global
| — | Connectionist (4–6) | Hierarchical (7) | Global (8) |
|---|---|---|---|
| Camp | localizationist | holist | holist |
| Unifying principle | discrete centres joined by connections | graded levels; higher modulate lower | ONE disturbed functional capacity |
| Number of factors | many components | multiple, ordered levels | a single overarching factor |
| Key figures | Broca, Wernicke, Lichtheim | Jackson, Jakobson, Brown | Marie (intelligence), Goldstein (abstract attitude) |
| Tie to evolution / development | weak / absent | central | secondary |
How each tradition explains the VARIETY of symptoms
| Tradition | Source of symptom variety |
|---|---|
| Connectionist (4–6) | WHICH centre or connection is damaged (a missing component). |
| Hierarchical (7) | WHICH LEVEL is lost; the brain performs at an integrated lower level. |
| Global (8) | the DEGREE / DOMAIN to which ONE general capacity is impaired. |
Both are holist reactions against connectionism (they reject discrete centres and invoke integrative factors); both descend from Jackson; and the boundary even blurs — Goldstein straddles both camps, accepting Jakobson's phonemic hierarchy while also positing a single global factor.
The clean differentiator: ONE disturbed capacity (global) vs MANY ordered LEVELS (hierarchical, tied to evolution/development). Their shared weakness: a general factor can't explain the specific, qualitative nature of language breakdown.
Strengths & the core weakness
| Strengths (credit them) | Weaknesses (the core problem) |
|---|---|
| Forced attention onto general psychological factors connectionism ignored (intelligence, abstract attitude, motivation, integration). | A single general factor can't explain the specific, qualitative nature of language breakdown, or the co-occurrence of particular symptoms. |
| Marie: revived the (ignored) comprehension deficit in Broca's aphasia; the vascular anatomy of the language zones; spurred detailed syndrome description. | Marie: never characterised "general intelligence"; comprehension disorders differ qualitatively; many deficits are purely linguistic. |
| Goldstein: a rich organismic view; clinical assessment of the abstract attitude; lasting concepts (diaschisis, catastrophe-avoidance, performance variability). | Goldstein: how can one loss yield both anomia (content words) and agrammatism (function words)? He admitted domain-specific breakdown & accepted localization. |
| The neural basis of such "general functions" is unclear — and whether they exist at all is debated (Fodor 1982). → Ch. 9 keeps the linguistic/psychological insights but rejects single-factor explanations. | |
Key-terms glossary
| Global / single-factor model | explains the variety of aphasic signs via one disturbed functional capacity. |
| Anarthria | Marie's subcortical motor speech disorder — a disorder of articulation, not of language. |
| Quadrilateral space / lenticular zone | the deep white-matter region (near the lenticular nucleus, between lines A & B) where, per Marie, a lesion causes anarthria. |
| General intelligence | Marie's unifying factor; tested by three-part commands; later tied to language + "ideas learned in a didactic fashion." |
| Organismic view | Goldstein's treatment of the patient as an integrated whole striving to cope and avoid catastrophe. |
| Abstract attitude | the conceptual / categorical stance (vs the concrete); its loss drives aphasic symptoms (Goldstein). |
| Concrete attitude | being passively bound to the immediate, specific situation. |
| Catastrophe / protective mechanisms | a failure marked by disorder/anxiety, which the patient avoids via orderliness & structure → explains performance variability. |
| Diaschisis | a damaged area's remote influence on intact tissue (von Monakow 1914) → Goldstein's "indirect" symptoms. |
| "Central" aphasia | Goldstein's term (a disturbance of inner speech) ≈ the connectionists' conduction aphasia. |
| De-differentiation | Goldstein/Jacksonian idea: the lesioned nervous system regresses to a less differentiated mode of function. |
| Iconoclast | Head's (1926) label for Marie — one who cast doubt on the connectionist taxonomies. |
| Holism | the view that integrated / unitary processes — not discrete centres — underlie language. |
Names & dates
| Pierre Marie 1906 (+1908) | "only one aphasia"; general intelligence; anarthria & the quadrilateral space; the vascular argument; the slogan. |
| Moutier 1908 | the vast thesis supporting Marie (387 + 44 cases; serial sectioning). |
| Marie–Dejerine discussions 1908 | Klippel 1908; Augusta Klumpke Dejerine's anatomical refutation (Broca's area lateral, not anterior; fibres pass through the quadrilateral). |
| Kurt Goldstein 1948 | Language and Language Disturbances; gestalt / organismic view; the four mechanisms; the abstract attitude. |
| Background | von Monakow 1914 (diaschisis); Vygotsky 1939 (inner speech); Geschwind 1964; Head 1926 ("iconoclast"); Fodor 1982 (do general functions exist?). |
The global models explain all aphasia by one disturbed capacity. Marie (1906) said there is only one aphasia — Wernicke's, a disorder of general intelligence — and that Broca-type output is a separate subcortical anarthria ("Broca's = Wernicke's + anarthria"), an argument undone in the 1908 controversy with Dejerine. Goldstein (1948), drawing on gestalt psychology, traced aphasic symptoms to the loss of the abstract attitude. Both rightly stressed general psychological factors, but neither could explain the specific nature of language breakdown — which is why the field moved on to the process models of Chapter 9.
Active-Recall Self-Test
Don't re-read — retrieve. Answer each out loud (or on paper), then click to reveal. ★ = high-yield.